 CONTACT US
CONTACT US
Dr Nico Coetzee
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Nico Coetzee
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Nico Coetzee
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Nico Coetzee
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
BREAST SURGERY
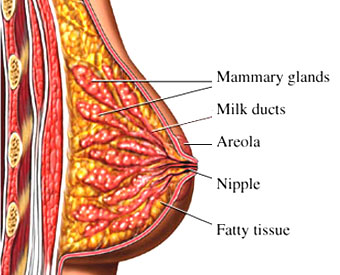
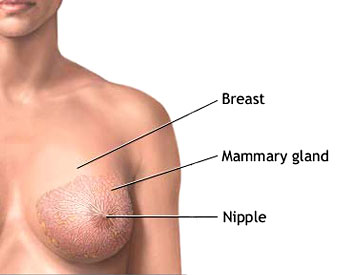
The female breast is composed mainly of fatty tissue interspersed with fibrous or connective tissue. The circular region around the nipple is often a different color or pigmented. This region is called the areola.
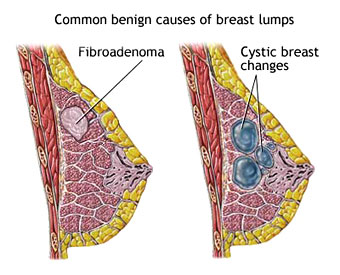
Causes of breast lumps
Fibro adenoma
Cystic breast changes
Malignancy
Self-
Self-
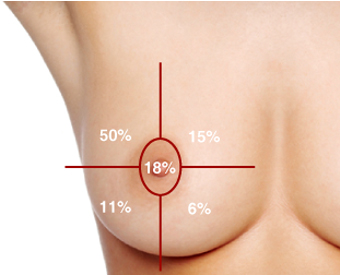
breast regions on the following points:
Visual inspection
Changes in skin texture
Retraction or indentation of nipple
Discharge from the nipple
Atypical fullness or puckering of the breast
Patients should do routine self-


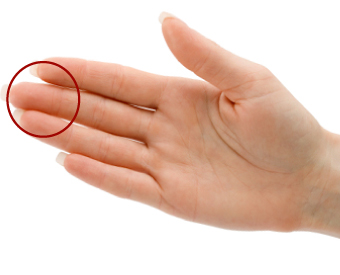

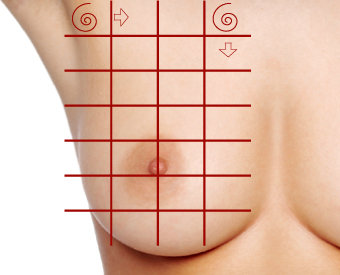














Superficial pressure














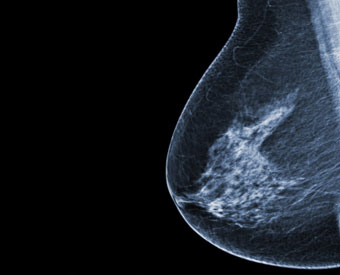
Mammogram
Mammography remains the gold standard for breast diagnostics.
Most radiology department use digital mammography.
Ultrasound and MRI may be used by the radiologist compliment mammography.
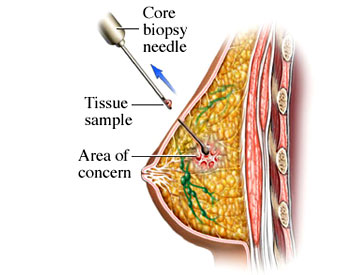
Needle Biopsy
A needle is used to draw fluid or tissue samples from the breast. This is called “fine needle aspiration cytology” and refers to the way the pathologist will examine the sample. Core needle biopsy will take a thicker tissue sample from the breast. These procedures are done in the consulting room.
Breast lump removal
Alternative Names
Lumpectomy; Wide local excision; Excisional biopsy; Limited breast surgery; Segmental mastectomy: Breast conservation therapy or surgery; Tylectomy; Breast sparing surgery; Partial mastectomy; Segmental breast excision
What is the breast lump removal procedure?
Breast lump removal is surgery to remove a lump in the breast and some surrounding tissue from the breast. Breast lump removal is usually done in an outpatient clinic.
You will be given general anesthesia (asleep, but pain free) or local anesthesia (awake, but sedated and pain free). The procedure takes about 1 to 2 hours.
The surgeon makes a small incision (cut) on your breast. The surgeon then removes some of the lump and breast tissue around it.
If the lump is not breast cancer, your surgeon will not remove very much breast tissue from around the lump.
If you have breast cancer, the amount of breast tissue around the lump the surgeon removes may depend on what type of breast cancer you have.
he surgeon will close the skin with stitches. These may dissolve or need to be removed later. A drain tube may be placed to remove excess fluid.
Your doctor will send the lump to a laboratory for testing. If you have a lump with breast cancer in it, your surgeon will also remove lymph nodes in your axilla (armpit). This will be done through another surgical cut underneath your arm. The lymph nodes will also be tested for cancer. This is called staging. Staging helps your doctor plan your treatment.
Why the Procedure Is Performed?
Lumpectomy is performed to either diagnose or treat an abnormal spot in the breast. Before a lumpectomy, your doctor will have done a needle biopsy and imaging tests (such as mammography ) to see if you have breast cancer. If a needle biopsy showed that you have breast cancer, your doctor will have you take more tests to see if the cancer has spread.
Treatment depends on the type of breast cancer, if the cancer has spread, and to where, your age, whether you have reached menopause, and your overall health.
For some breast cancer, mastectomy may be better treatment. For other breast cancer, lumpectomy (breast conservation therapy) may treat your cancer. Your doctor will help you decide what treatment is best for you .
Other reasons to perform a lumpectomy are:
If you have fibroadenoma or other benign tumors of the breast.
If you have a fluid-
Breast Cancer
Breast cancer is a cancer that starts in the tissues of the breast. There are two main types of breast cancer:
Ductal carcinoma starts in the tubes (ducts) that move milk from the breast to the nipple. Most breast cancers are of this type.
Lobular carcinoma starts in the parts of the breast, called lobules, which produce milk.
In rare cases, breast cancer can start in other areas of the breast. Breast cancer may be invasive or noninvasive. Invasive means it has spread from the milk duct or lobule to other tissues in the breast. Noninvasive means it has not yet invaded other breast tissue. Noninvasive breast cancer is called “in situ.”
Ductal carcinoma in situ (DCIS), or intraductal carcinoma, is breast cancer in the lining of the milk ducts that has not yet invaded nearby tissues. It may progress to invasive cancer if untreated.
Lobular carcinoma in situ (LCIS) is a marker for an increased risk of invasive cancer in the same or both breasts.
Many breast cancers are sensitive to the hormone estrogen. This means that estrogen causes the breast cancer tumor to grow. Such cancers have estrogen receptors on the surface of their cells. They are called estrogen receptor-
Some women have what’s called HER2-
Alternative Names: Cancer – breast; Carcinoma – ductal; Carcinoma – lobular; DCIS; LCIS; HER2-
- Causes, Incidence, And Risk Factors
- Over the course of a lifetime, 1 in 8 women will be diagnosed with breast cancer.
- Risk factors you cannot change include:
Age and gender — Your risk of developing breast cancer increases, as you get older. Most advanced breast cancer cases are found in women over age 50. Women are 100 times more likely to get breast cancer than men.
Family history of breast cancer — You may also have a higher risk for breast cancer if you have a close relative who has had breast, uterine, ovarian, or colon cancer. About 20 – 30% of women with breast cancer have a family history of the disease.
Genes — Some people have genes that make them more likely to develop breast cancer. The most common gene defects are found in the BRCA1 and BRCA2 genes. These genes normally produce proteins that protect you from cancer. If a parent passes you a defective gene, you have an increased risk for breast cancer. Women with one of these defects have up to an 80% chance of getting breast cancer sometime during their life.
Menstrual cycle — Women who got their periods early (before age 12) or went through menopause late (after age 55) have an increased risk for breast cancer.
Other risk factors include:
Alcohol use — Drinking more than 1 – 2 glasses of alcohol a day may increase your risk for breast cancer.
Childbirth — Women who have never had children or who had them only after age 30 have an increased risk for breast cancer. Being pregnant more than once or becoming pregnant at an early age reduces your risk of breast cancer.
DES — Women who took diethylstilbestrol (DES) to prevent miscarriage may have an increased risk of breast cancer after age 40. This drug was given to the women in the 1940s – 1960s.
Hormone replacement therapy (HRT) — You have a higher risk for breast cancer if you have received hormone replacement therapy with estrogen for several years or more. Obesity — Obesity has been linked to breast cancer, although this link is controversial. The theory is that obese women produce more estrogen, which can fuel the development of breast cancer.
Radiation — If you received radiation therapy as a child or young adult to treat cancer of the chest area, you have a much higher risk for developing breast cancer. The younger you started such radiation and the higher the dose, the higher your risk — especially if the radiation was given during breast development.
Breast implants, using antiperspirants, and wearing underwire bras do not raise your risk for breast cancer. There is no evidence of a direct link between breast cancer and pesticides.
Symptoms
Early breast cancer usually does not cause symptoms. This is why regular breast exams are important. As the cancer grows, symptoms may include:
Breast lump or lump in the armpit that is hard, has uneven edges, and usually does not hurt
Change in the size, shape, or feel of the breast or nipple — for example, you may have redness, dimpling, or puckering that looks like the skin of an orange
Fluid coming from the nipple — may be bloody, clear to yellow, green, and look like pus
Men can get breast cancer, too. Symptoms include breast lump and breast pain and tenderness.
Symptoms of advanced breast cancer may include:
- Bone pain
- Breast pain or discomfort
- Skin ulcers
- Swelling of one arm (next to the breast with cancer)
- Weight loss
Signs And Tests
The doctor will ask you about your symptoms and risk factors. Then the doctor will perform a physical exam, which includes breasts, armpits, and the neck and chest area.
Tests used to diagnose and monitor patients with breast cancer may include:
- Breast MRI to help better identify the breast lump or evaluate an abnormal change on a mammogram
- Breast ultrasound to show whether the lump is solid or fluid-
filled - Breast biopsy, using methods such as needle aspiration, ultrasound guided, stereotactic, or open
- CT scan to see if the cancer has spread
- Mammography to screen for breast cancer or help identify the breast lump
- PET scan
- Sentinel lymph node biopsy to see if the cancer has spread
If your doctor learns that you do have breast cancer, more tests will be done to see if the cancer has spread. This is called staging. Staging helps guide future treatment and follow-
Treatment
Treatment is based on many factors, including:
- Type and stage of the cancer
- Whether the cancer is sensitive to certain hormones
- Whether the cancer overproduces (overexpresses) a gene called HER2/neu
In general, cancer treatments may include:
Chemotherapy medicines to kill cancer cells
Radiation therapy to destroy cancerous tissue
Surgery to remove cancerous tissue — a lumpectomy removes the breast lump; mastectomy removes all or part of the breast and possible nearby structures
Hormonal therapy is prescribed to women with ER-
An example of hormonal therapy is the drug Tamoxifen. This drug blocks the effects of estrogen, which can help breast cancer cells survive and grow. Most women with estrogen-
Another class of hormonal therapy medicines called aromatase inhibitors, such as Exemestane (Aromasin), has been shown to work just as well or even better than Tamoxifen in postmenopausal women with breast cancer. Aromatase inhibitors block estrogen from being made.
Targeted therapy, also called biologic therapy, is a newer type of cancer treatment. This therapy uses special anticancer drugs that target certain changes in a cell that can lead to cancer. One such drug is Trastuzumab (Herceptin). It may be used for women with HER2-
Cancer treatment may be local or systemic.
Local treatments involve only the area of disease. Radiation and surgery are forms of local treatment.
Systemic treatments affect the entire body. Chemotherapy is a type of systemic treatment.
Most women receive a combination of treatments. For women with stage I, II, or III breast cancer, the main goal is to treat the cancer and prevent it from returning (curing). For women with stage IV cancer, the goal is to improve symptoms and help them live longer. In most cases, stage IV breast cancer cannot be cured.
Stage 0 and DCIS — Lumpectomy plus radiation or mastectomy is the standard treatment. There is some controversy on how best to treat DCIS.
Stage I and II — Lumpectomy plus radiation or mastectomy with some sort of lymph node removal is the standard treatment. Hormone therapy, chemotherapy, and biologic therapy may also be recommended following surgery.
Stage III — Treatment involves surgery, possibly followed by chemotherapy, hormone therapy, and biologic therapy.
Stage IV — Treatment may involve surgery, radiation, chemotherapy, hormonal therapy, or a combination of these treatments.
After treatment, some women will continue to take medications such as tamoxifen for a period of time. All women will continue to have blood tests, mammograms, and other tests after treatment.
Women who have had a mastectomy may have reconstructive breast surgery, either at the same time as the mastectomy or later.
Support Groups
Talking about your disease and treatment with others who share common experiences and problems can be helpful.
Expectations (Prognosis)
New, improved treatments are helping persons with breast cancer live longer than ever before. However, even with treatment, breast cancer can spread to other parts of the body. Sometimes, cancer returns even after the entire tumor is removed and nearby lymph nodes are found to be cancer-
How well you do after being treated for breast cancer depends on many things. The more advanced your cancer, the poorer the outcome. Other factors used to determine the risk for recurrence and the likelihood of successful treatment include:
- Location of the tumor and how far it has spread
- Whether the tumor is hormone receptor-
positive or - negative - Tumor markers, such as HER2
- Gene expression
- Tumor size and shape
- Rate of cell division or how quickly the tumor is growing
After considering all of the above, your doctor can discuss your risk of having a recurrence of breast cancer.
Complications
You may experience side effects or complications from cancer treatment. For example, radiation therapy may cause temporary swelling of the breast (lymphedema), and aches and pains around the area.
Lymphedema may start 6 to 8 weeks after surgery or after radiation treatment for cancer.
It can also start very slowly after your cancer treatment is over. You may not notice symptoms until 18 to 24 months after treatment. Sometimes it can take years to develop.
Ask your doctor about the side effects you may have during treatment.
When to call your Doctor?
Contact surgeon for an appointment if:
- You have a breast or armpit lump
- You have nipple discharge
Also call Doctor Coetzee if you develop symptoms after being treated for breast cancer, such as:
- Nipple discharge
- Rash on the breast
- New lumps in the breast
- Swelling in the area
- Pain, especially chest pain, abdominal pain, or bone pain
Prevention
Tamoxifen is approved for breast cancer prevention in women aged 35 and older who are at high risk. Discuss this with your doctor. Women at very high risk for breast cancer may consider preventive (prophylactic) mastectomy. This is the surgical removal of the breasts before breast cancer is ever diagnosed. Possible candidates include:
Women who have already had one breast removed due to cancer
Women with a strong family history of breast cancer
Women with genes or genetic mutations that raise their risk of breast cancer (such as BRCA1 or BRCA2)
Your doctor may do a total mastectomy to reduce your risk of breast cancer. This may reduce, but does not eliminate the risk of breast cancer. Many risk factors, such as your genes and family history, cannot be controlled. However, eating a healthy diet and making a few lifestyle changes may reduce your overall chance of getting cancer.
There is still little agreement about whether lifestyle changes can prevent breast cancer. The best advice is to eat a well-
Choose foods and portion sizes that promote a healthy weight
Choose whole grains instead of refined grain products
Eat 5 or more servings of fruits and vegetables each day
Limit processed and red meat in the diet
Limit alcohol consumption to one drink per day (women who are at high risk for breast cancer should consider not drinking alcohol at all)


