CONTACT US
CONTACT US
Dr Nico Coetzee
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Nico Coetzee
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Nico Coetzee
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
Dr Coetzee specializes in Laparoscopic and Open surgery including certain areas of Surgical Oncology
Dr Nico Coetzee
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Coetzee joined the Medi Clinic group at Somerset West in 2009..Previously active and involved in the evolution of Laparoscopic Surgery as a participant and as an educator at Tygerberg Hospital in the Western Cape.
Dr Nico Coetzee
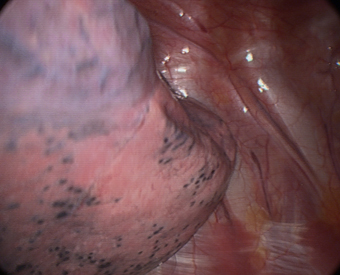
BILATERAL CERVICAL SYMPATHECTOMY
With gravity the lung naturally falls downwards and away from the upper posterior chest wall. Only one 7mm or 10mm port with an operative-
We perform bilateral synchronous sympathectomy starting on the right side. An l-
Care should be taken not to divide the sympathetic chain above the level of the second rib for the treatment of palmar and plantar hyperhidrosis, because it increases the risk of Horner’s syndrome and contributes little benefit. Thoracic outlet syndrome or reflex sympathetic dystrophy is usually approached at t1-
Any shortness of breath or swelling at the operation site should be discussed with Doctor Coetzee.
This website is not intended to take the place of your discussion with your surgeon about the need for surgery. If you have questions about your need for surgery, your alternatives, billing or insurance coverage, or your surgeons training and experience, do not hesitate to ask Doctor Coetzee or his office staff about it.
Patient selection
Surgical interruption of intrathoracic autonomic neural pathways has several useful clinical applications, particularly thoracic sympathectomy for upper limb hyperhidrosis. (severe sweating of the hands and axillae.) Most patients with severe sweating of the hands and under the arms will benefit by this procedure.
Operative steps
Surgical techniques: general anesthesia is used, including one lung ventilation with a double lumen endobronchial tube. Co 2 insufflation is used to help induce lung collapse. A semi-